
The thought of nursing clinics may put the fear factor into some nurses’ shifts. The author firmly believes, therefore, for patients’ well-being and to maintain the client-owner bond and individual nurse’s well-being, these should be optional.
Think of your own experiences – a negative event can often lead to refusing to subject ourselves to the same demoralising situation again. Very rarely when faced with a pushy sales person or feeling undervalued as a customer do you return to the same store. The same outcome can occur in practice; a rule of “one strike and you are out” approach from clients exists.
A client told by a vet “your dog is fat” will often request a different vet next time or be reluctant to follow advice given. The same can arise with clinics – owners who do not feel their needs are being addressed or who feel patronised or scolded in any way will often not return. Therefore, for clinics to succeed it is vital the right nurses are involved. The opportunity for any nurse to venture into clinics (should one choose to) should always be available.
Some nurses may dread clinics as they feel “I have not had enough training”, which may be the case. Putting a nurse into such a scenario without the support they need can cause stress, lead to self doubt and uncertainty and significantly affect job satisfaction. This creates issues retaining staff and places overall pressure on a practice.
Practice training – whether online courses, in-house or both – is, for this author, a must and recommended for all clinic nurses. Practices should also offer further support using a check in-type process that allows nurses the opportunity to discuss any elements that may have come to light since conducting clinics.
Another common fear is “what if I’m asked something I don’t know the answer to?” How can we avoid this pitfall? The simple answer is we are not expected to know all the answers all of the time, but these scenarios are actually important for development. However, the manner we address the answers in, and the deliverance, will determine whether an owner feels they can trust us.
The worst thing we could do is guess an answer. An owner may be embarrassed to have asked a question in the first instance, or may actually know the answer and wish to question our professional response. How often will you hear a remark such as “the owner is a doctor; nurse; surgeon; specialist”. We don’t know every owner’s occupation, nor should we have to know, because it should not be a factor. Remaining honest and professional to all clients and maintaining the five main principles of practice set out by the code of conduct is mandatory1. Let the client know if you are unaware and you can find out.
This author does not know all the answers, but knowing the answers and refraining from voicing them is also a daily occurrence for nurses. As nurses, we cannot legally provide all the answers. In certain situations, a simple yes or no could suggest a diagnosis or treatment plan, which could lead to disciplinary action for a nurse.
Yet, with many owners still, sadly, having little or no idea about the amount of support and knowledge nurses have, this author understands and wishes to highlight to the public that nurses are not glorified kennel maids (interestingly, how this author started out), but qualified, professional individuals. We wish to support the longevity and health of clients’ pets and their (pet-human) bond wherever we can, and clinics provide such an environment.
Over the years as nurses, we expand our professional knowledge. For example, in a scenario of a telephone call consisting of “my dog is trying to vomit”, alarms bells of foreign body, acute poisoning, gastric dilatation volvulus and so on may ring, so we proceed to ask questions pertaining to such causes to gain as much information as possible (without hinting potential concerns). We start to scan the breed and age, and list all the possibilities (internally) while remaining calm. Asking “has the dog eaten anything she shouldn’t have?” may be something you do now or will come with experience.
You opted for a career where the patient cannot provide you with any information. It is your nursing skills, knowledge and experience that will support you in numerous aspects of your role, and this includes clinics.
Not all consultations are positive and productive, and one being executed differently next time may help. A negative consult should not be feared, but viewed as a challenge to re-evaluate. A vast undercurrent of psychology is involved in consulting – another understandable source of dread for some nurses. For some, it may appear easy to read a room, or misjudge a client’s personality trait, which is okay, too. It’s how you gauge the remainder of the consultation.
Think about your body posture and your tone. Have you faced the computer taking notes for too long and not engaged enough with the patient? Sitting on the floor with the patient, or merely interacting – having taken into account the patient’s body language (as this is not always suited to every scenario) – may help put an owner at ease, but read the patient as well as the room. The owner’s behaviour often impacts the pet.
The patient-owner bond can be extremely strong; dependency, support and companionship must be acknowledged. A client must feel they can trust you and your advice to achieve compliance. Ask yourself “would I be happy with the service?”. If the answer is a resounding “yes”, could you be used to support others within the practice with training or mentoring and so on? If the answer is unclear or “no”, it should not be viewed negatively. As you’ve identified an area of interest, other nurses may feel the same.
Does the practice need to improve its training? Under the mnemonic SUPERB, which covers Schedule 3 delegation, vets need to question:
- Experience – does the RVN/SVN feel capable, and have sufficient competence and expertise?
- Be there – are you [your veterinary surgeons] available to direct or supervise as necessary?2
Nurse clinics can cover a vast array of topics. This author strongly believes all new pets should be requested to attend a nurse “new to practice” consultation. It is important not only for the client to glimpse the practice (equipment and products), but the support offered. It is not a hard-hitting sales pitch; we do not need to bombard clients with information. It is, however, an opportunity to assess how we can best support an individual. Is this a first-time pet? What happened to their last pet? Is there a reason this specific pet was chosen? Approach the conversation as we would any emergency telephone call, actively listening to vital details and internalising possibilities.
Some clients will share information with you, while some will not. This may also be down to the setting of the consultation, and if they feel valued and supported. It is not for every client and some may take time, but only if the initial consultation is a success.
Consultations: 10 touch points

The author began consult training during her student days, under the wisdom and guidance of her clinical coach Mary Crease, who installed “10 touch points of a pet conversation” (which the author still uses today). Regardless of species or life stage, these 10 topic areas allow for a guided consultation and structure that allow the nurse to identify any potential concerns or areas of interest to report to a vet for further instruction (Figure 1).
Whether the clinic is for a new pet, obesity or general wellness, touch points will remain the same, but the depth and investigation into certain points will change depending on the consultation.
Every clinic can cover a multitude of areas in quick succession with a mere question. The depth of each answer can highlight where the focus lies in terms of future clinics. For example, from a new puppy to a geriatric cat, exercise and mental stimulation will remain important. Identifying potential aspects of pain or boredom that a client may or may not have noticed can be investigated by simply asking “what does your pet do for exercise?”
Simple open questions can reveal so much, but remember not all owners welcome advice, so adapting your consultation style on an individual basis may increase productivity. “You mentioned that Tommy’s nails are long, would you like some information on keeping them short?”. This example would allow you to discuss exercise, changes to routine and keep an open dialogue.
In a geriatric cat, pain associated with the long nails may have led to reduced activity and sleeping more, rather than attempting to walk to disguise pain. Potentially, any number of the 10 points could be impacted, including toilet habits and bodyweight – a number of reasons the owner may be struggling with or unaware of.
Passive-aggressive questions or comments, such as “why are Tommy’s nails so long?” or “Tommy’s nails are too long”, can easily shut down a client’s response, and Tommy may leave the consult with long nails, so no one wins. Questions and statements must be free of disadvantage, discrimination or bias to succeed.
Some answers may lead to a closed response – “no, thank you” – which is fine. The offer to discuss was made should the owner wish to enquire in future. Never push advice.
Enquiring about eating, drinking, urinating and faecal habits (EDUF) can change the simplest of consults on to any number of additional questions or avenues, but bear in mind every question needs to provide you with an answer you must use.
For a new pet, owners generally want to show off their new addition. Identify something – anything – you like about the animal. Use your imagination, if required. This tool is key; it will allow you to discover how much the owner is willing to share or it may lead on to a conversation about the litter. Remember, actively listen at all times. Does something sound wrong to you? Also, remember puppy farms are not a myth and not all animals are bred in loving homes, including cats.
Gauge the pet’s interaction. If it’s an older pet, it may have been into several homes first or with the family the whole time.
The owner’s response will often dictate how the consultation will go. If an owner does not wish to share or engage, it may be they are nervous or anxious, or they feel on trial. If so, as professionals, we may need to alter our approach.
How is the owner presenting body language-wise or in their vocal tone? While our body language should be open, a soft, quietly spoken owner may appreciate a similar tone from us. This is not to be regarded as patronising, but using the consult the best you can by reading the room will allow clients to gauge their next response.
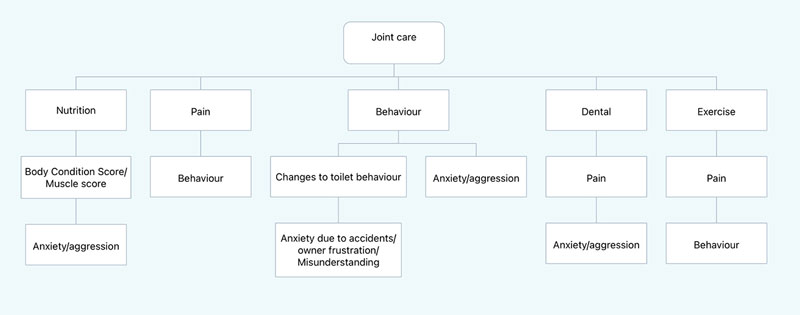
After enquiring about EDUF, were any concerns raised regarding toilet habits, frequency, location, vocalising, or owner concerns, such as the patient starting to urinate inside the house? Could it be a joint-related issue? (Figure 2).
Is the floor too slippery to get outside? Has a new cat moved into the area causing territorial issues? Is anxious behaviour in a dog due to noise? Use all of your CPD, what could it be? How can the question rule out or provide more information?
Remember, at all times, it is not for veterinary nurses to discuss a potential diagnosis or predict treatment. Any phrase that could be deemed by an owner as a future diagnosis could detrimentally impact your future as an RVN.
Make sure you remain compliant in your role at all times. For example, for an owner who makes the comment “I think Bob has arthritis”, a nurse should always err on the side of caution and reply such as “I can see Bob found it difficult to get up from that position”. A simple “yes” to the owner could be deemed as a diagnosis by a nurse. If, however, a vet had diagnosed arthritis in a patient’s clinical exam then you would be covered legally.
If the nurse has observed a stiff gait in the pet, ask the owner if they would like home support for Bob. You might receive a “yes please”, which is great or, unfortunately, an “oh it’s his age”. In these situations, “keep calm and carry on vet nursing”. Calmly explain to owners human conditions differ from pet conditions and that a vet can discuss this with them. The vet will open the discussion of a multimodal approach to joint care, diet, exercise, laser therapy and, subsequently, an additional clinic.
You will not be able to convince every owner and not all owners can afford high-end veterinary treatments. Listen to what each owner is telling you.
If no concerns with EDUF arise, lead on to neutering. Questions such as “when are you going to neuter?” or “are you going to breed?” may be perceived by some owners as intrusive. “Any thoughts on neutering?” may be an easier way of asking and remaining neutral. Such a question also adds validity to the owner’s response and opens up the conversation if they are unaware of what to do.
If unsure on how you should respond, your practice should have its own set policy or protocol regarding neutering. It is often a hot debate with some owners, so if you feel unable to answer, be honest and let the client know you can arrange for a vet to speak to them regarding the issue, should they wish.
If you have concerns over diet or a patient’s weight (underweight or overweight), enquire about nutrition. Some owners are often grateful you asked, as they want to know how good the food is or if it is the right amount.
If your clinic is linked to a particular brand, let them know. This links in nicely with your practice’s health club plan (if it provides a discount for the food). It’s not a hard sell – just planting a “thought seed”, such as “we would recommend xxx. Our pet health club members also receive a discount on food purchased in practice”.
For neutered pets or owners who are going to neuter, inform them of the metabolic changes post-neutering, and the decrease in the pet’s ability to use the food. Assure them nurses can help, should the owner need it.
If the pet looks underweight, enquire about dental care, any drooling or halitosis. This could lead into a preventive treatment question, such as which products are used, or educating on available products, from dental support to parasitic treatments.
Many owners are unaware of the flea life cycle and how the tapeworm life cycle feeds into it, so a very brief recap on how tapeworm eggs are ingested by flea larvae can do the trick. Explain to owners this is why they are advised to treat for fleas and worms at the same time, rather than some believing it’s a sales tactic.
Is the pet’s weight a concern that may need the attention of a vet? Would the pet require the support of a weight clinic? How do you feel the owners would respond to this suggestion? Having actively listened, has the owner made you aware of something so far that would trigger assistance from you? For example, were joints or nails mentioned, or any lack of activity? Any one of these could be supported with an obesity clinic (Figure 2).
Some owners may feel judged when it comes to an animal’s weight, so careful wording is required. Any form of judgement on your part will prevent the patient from receiving your help – the reason why so many of us are in this industry. However, it is not always that simple. As this author knows, some owners will remain blissfully unaware of what the extra weight is doing to their pet, so even a gentle change may help.
Commandeer any opportunity to educate the public on pet insurance. A practice leaflet or link for the owner to refer to, or case studies in reception to highlight costs, could be beneficial.
Yet another minefield to overcome is which insurance company to use. Remember, under the Financial Conduct Authority guidelines, we can only comment on our own personal polices, such as “that suited my circumstances”. We cannot legally recommended a type of policy, let alone which insurance companies to avoid.
We can, however, recommend owners read the small print and explain what a pre-existing condition means to an insurance company, but be careful. Do not dwell on a point if it is not relevant.
The author highly recommends a quick mention on the importance of updating information on a microchip, scanning in front of the owner to confirm the chip is present.
Scanning can indicate one of three things:
- no chip present
- chip is present, but owner was not aware
- a chip is present and the owner’s details are correct
Get into the habit (if your practice has not already) of chip checking. A microchip can be a matter of life and death, with the potential to save and reunite so many pets effectively.
During clinical observations and under Schedule 3 of the Veterinary Surgeons Act, an RVN is legally allowed to comment on aspects they see, palpate, smell or hear during a consultation. However, any findings deemed abnormal must be recorded as such on the patient’s record and no further discussion regarding the findings must be made3. Discussions would be deemed potential diagnosis and illegal under the said act.
For example, if during a new patient clinic physical exam on a two-year-old entire male Staffordshire bull terrier you palpate only one descended testicle, you can say it is abnormal, as male dogs should have two testicles, but you cannot say the patient would require surgery or the potential health risks associated with the condition, as this would involve diagnosing or a potential treatment or course of action.
Inform the owner you recommend they book an appointment to discuss the matter with a vet.
In summary
Always recap with a client what you are going to do. Whether it is speaking to a vet, or providing additional reading material or links to support sites, confirm information received during the clinic and for next time (if any is advised) and walk the client back out to reception. Once the client has paid they will often have a question. If you are there, this prevents them leaving unsure or forgetting to ask.
The author strongly believes clinics should be a paid-for service; it places value on your knowledge, status and the service the client receives. If you feel you are not providing a service worthy of payment then question is it due to a lack of training or support?
Nurse clinics need to be used and viewed as routine appointments, normalising health check opportunities for the client to check in with the practice. This should provide the opportunity for owners to know what is normal for their pet and educate them on signs to look out for.
The author hopes if you have the drive and passion to conduct clinics, or you feel you may enjoy clinics and educating clients, you receive support and training, as you are an asset to any practice.
Leave a Reply